Troponin in Myocardial Infarction: How to Interpret Rising and Falling Values
Description: A practical guide to interpreting troponin in myocardial infarction, including the 99th percentile, rise-and-fall patterns, serial testing, STEMI vs NSTEMI, and common non-ischemic causes of elevated troponin.

|
Quick answer: Troponin is the preferred blood biomarker for detecting myocardial injury. In myocardial infarction, the key pattern is a rise and/or fall in troponin with at least one value above the 99th percentile upper reference limit, plus evidence of acute myocardial ischaemia such as symptoms, new ischaemic ECG changes, imaging evidence, or angiographic proof of coronary thrombosis. A positive troponin does not automatically mean type 1 MI; serial testing and clinical context are essential. |
Few laboratory tests are as important in acute cardiology as cardiac troponin. For medical students and junior doctors, troponin can seem simple at first: if it is elevated, think myocardial infarction. In real practice, however, troponin interpretation is more nuanced. Troponin identifies myocardial injury, but it does not tell you the cause on its own. That distinction matters because a patient with plaque rupture and acute coronary occlusion needs a different response from a patient with sepsis, pulmonary embolism, myocarditis, tachyarrhythmia, or chronic kidney disease.
The safest way to interpret troponin is to combine three elements: the absolute value, the pattern over time, and the clinical context. In other words, you should not ask only “Is the troponin high?” You should also ask “Is it rising or falling?” and “Does the patient have evidence of acute myocardial ischaemia?” Once you approach troponin this way, confusing cases become much easier to reason through.
What troponin actually measures
Cardiac troponin I and cardiac troponin T are structural proteins found within myocardial cells. When myocardial cells are injured, troponin is released into the circulation. Because these proteins are highly specific to the heart, they are the preferred biomarkers for detecting myocardial injury. Modern high-sensitivity cardiac troponin assays can detect very small amounts of troponin and therefore identify injury earlier than older assays.
This increased sensitivity is clinically useful, but it also creates a trap for beginners. A troponin result above the reference threshold proves myocardial injury, not necessarily myocardial infarction. Myocardial infarction is a specific clinical diagnosis that requires myocardial injury plus evidence of acute myocardial ischaemia. That extra step is crucial.
The 99th percentile: the number every junior doctor should know
The universal definition of myocardial infarction states that myocardial injury is present when cardiac troponin is above the 99th percentile upper reference limit for the assay being used. That means your hospital’s assay-specific threshold matters. Different laboratories may use different assays, and those assays can have different numerical cutoffs. As a result, safe interpretation begins with knowing the local troponin assay and its decision threshold.
High-sensitivity troponin assays are now preferred because they improve early detection of myocardial injury. Major guidance also emphasises that clinicians should know the analytical performance of the assay used at their institution and, where applicable, understand sex-specific 99th percentile limits. In plain terms: do not rely on memory from another hospital or another textbook. Use the threshold that belongs to the assay in front of you.
Why the rise-and-fall pattern matters
A single troponin value is only a snapshot. To diagnose acute myocardial infarction, clinicians usually need a dynamic change, meaning a rise and/or fall over time. This helps distinguish acute injury from chronic myocardial injury. A patient with chronic structural heart disease or chronic kidney disease may have a persistently elevated troponin without an acute infarction. By contrast, an evolving acute coronary event typically shows a changing pattern on serial sampling.
The exact delta used in clinical pathways depends on the assay and the protocol adopted by the institution. Some pathways focus on absolute changes; others use relative changes in selected situations. The practical bedside lesson is simple: if the clinical question is myocardial infarction, a repeat troponin is usually as important as the first one.

Myocardial injury is not always myocardial infarction
The Fourth Universal Definition of Myocardial Infarction draws an important distinction. Myocardial injury exists when troponin exceeds the 99th percentile. Acute myocardial injury exists when there is a rise and/or fall in troponin. Acute myocardial infarction is a subset of acute myocardial injury in which there is also evidence of myocardial ischaemia. Without evidence of ischaemia, the correct label is myocardial injury rather than infarction.
This distinction prevents two common mistakes. The first is over-calling myocardial infarction in any sick patient with a positive troponin. The second is dismissing positive troponin values as meaningless just because the patient does not have textbook chest pain. Elevated troponin outside acute coronary syndrome is often clinically important and may carry a worse prognosis, even when it is not caused by type 1 MI.
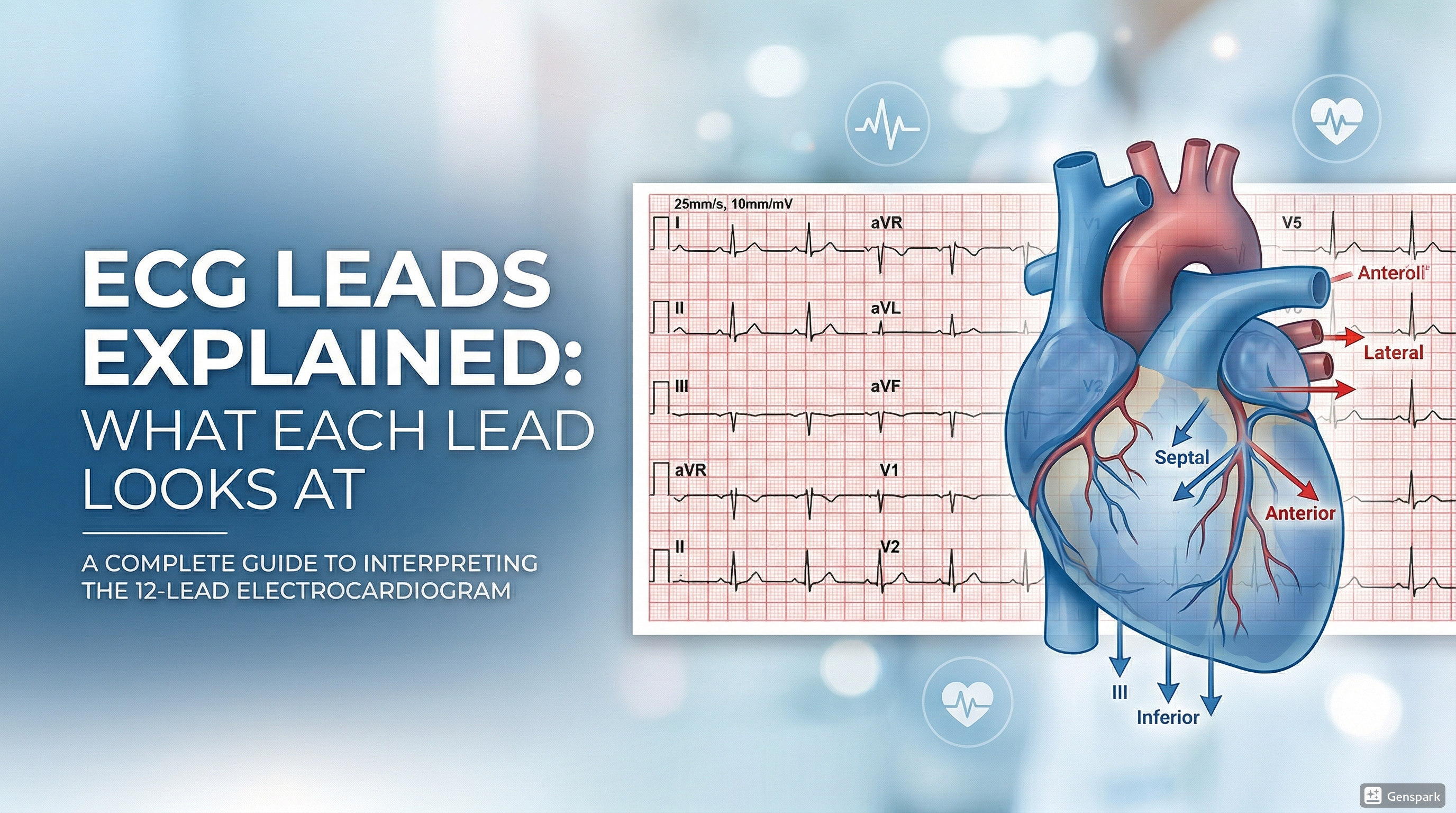
What turns an elevated troponin into acute myocardial infarction?
To diagnose acute MI, you need both biomarker evidence of acute injury and clinical evidence of ischaemia. The ischaemic evidence can come from symptoms of acute myocardial ischaemia, new ischaemic ECG changes, development of pathological Q waves, imaging evidence of new loss of viable myocardium or a new regional wall-motion abnormality, or identification of a coronary thrombus. In day-to-day practice, the diagnosis most often rests on symptoms, ECG findings, and serial troponin results considered together.
This is why troponin should never be interpreted in isolation. A patient with crushing central chest pain, dynamic ST changes, and a rising troponin has a very different problem from a septic patient with sinus tachycardia, a nonspecific ECG, and a modest troponin rise from supply-demand mismatch or non-ischaemic myocardial injury.
How troponin behaves in STEMI and NSTEMI
STEMI
In STEMI, diagnosis is usually driven by the ECG first. Persistent ST-segment elevation in a compatible clinical setting should trigger urgent reperfusion without waiting for troponin results to “confirm” the diagnosis. Troponin will usually rise, but treatment decisions in obvious STEMI are time-critical and should not be delayed while waiting for the lab.

NSTEMI
In NSTEMI, troponin plays a more central diagnostic role because the ECG does not show persistent ST elevation. Instead, the ECG may show ST depression, T-wave inversion, or may even be normal early on. Here, the combination of symptoms, serial ECGs, and serial troponins helps establish the diagnosis. A rising or falling troponin above the 99th percentile with evidence of ischaemia supports NSTEMI.

How serial troponin testing works in practice
Modern acute chest pain pathways often use high-sensitivity troponin at presentation and then repeat testing at a short interval, commonly 1 hour, 2 hours, or 3 hours depending on the validated local protocol. These pathways aim to identify patients at very low risk for acute MI, patients with clear rule-in patterns, and an intermediate group who need further observation or testing.
For junior doctors, the operational point is not to memorise every international algorithm word for word. It is to know which protocol your hospital uses and to follow it carefully. Ask: What time was the first sample taken? When is the repeat due? Is the patient still symptomatic? Has the ECG changed? The best troponin interpretation is always paired with accurate timing.

Common non-ischaemic and non-ACS causes of troponin elevation
Troponin can rise in many conditions outside type 1 myocardial infarction. Important cardiovascular causes include heart failure, tachyarrhythmias, myocarditis, pericarditis, acute aortic syndromes, severe hypertension, and stress cardiomyopathy. Non-cardiac causes include pulmonary embolism, sepsis, stroke, chronic kidney disease, severe gastrointestinal bleeding, rhabdomyolysis, and critical illness. Cardiac procedures, cardioversion, ablation, and blunt chest trauma can also raise troponin.
These are not “false positives.” They usually represent real myocardial injury, even if the mechanism is not plaque rupture with coronary thrombosis. That is why an elevated troponin outside ACS should not be ignored. Instead, it should prompt you to ask what process is injuring the myocardium and what the immediate clinical threat might be.
A simple bedside framework for interpreting troponin
When you review a troponin result, move through these questions in order:
- Is the troponin above the assay-specific 99th percentile upper reference limit?
- Is there a rising and/or falling pattern on serial measurements?
- Does the patient have symptoms or other evidence of acute myocardial ischaemia?
- What does the ECG show right now, and has it changed?
- Could this be STEMI, where reperfusion should not wait for biomarker confirmation?
- If it is not type 1 MI, what alternative cause of myocardial injury best explains the result?
This framework is deliberately basic, but it prevents most common interpretation errors. It also keeps the troponin result connected to the patient rather than to the laboratory number alone.
Common mistakes junior doctors make
- Calling every elevated troponin a myocardial infarction.
- Ignoring the timing of symptom onset and serial sampling.
- Waiting for troponin to confirm an obvious STEMI on ECG.
- Failing to consider alternative causes of myocardial injury in a sick inpatient.
- Using old or incorrect reference thresholds instead of the local assay-specific cutoff.
- Forgetting that a normal early troponin does not completely exclude MI if symptoms are very recent.
Clinical relevance for medical students and junior doctors
In exams, troponin is often presented as a neat diagnostic tool. In real life, it is a test that becomes powerful only when used correctly. If you understand the 99th percentile threshold, the importance of a rise-and-fall pattern, the need for evidence of ischaemia, and the broad differential diagnosis of myocardial injury, you will avoid many of the errors that trap inexperienced clinicians.
The most practical message is this: do not ask whether troponin is positive or negative. Ask what the troponin pattern means in this patient, at this time, with this ECG, and with this clinical story. That is the habit that turns a lab result into good clinical judgement.
Frequently asked questions
Does an elevated troponin always mean myocardial infarction?
No. It means myocardial injury. Myocardial infarction requires myocardial injury plus evidence of acute myocardial ischaemia.
Can troponin be normal early in myocardial infarction?
Yes. Very early after symptom onset, the first troponin may still be below the diagnostic threshold. That is why serial testing is important.
Should treatment of STEMI wait for troponin results?
No. In a clear STEMI, reperfusion decisions are driven by the ECG and clinical picture. Troponin should not delay urgent treatment.
Why do septic or critically ill patients often have raised troponin?
Critical illness can cause myocardial injury through mechanisms such as oxygen supply-demand imbalance, inflammation, hypotension, or direct myocardial stress.
What is the key role of serial troponin testing?
Serial testing helps distinguish acute evolving injury from chronic stable elevation and improves rule-in or rule-out decisions in suspected ACS.
Key takeaways
- Cardiac troponin I and T are the preferred biomarkers for myocardial injury.
- A value above the 99th percentile upper reference limit indicates myocardial injury, not automatically myocardial infarction.
- Acute myocardial infarction requires a rise and/or fall in troponin plus evidence of acute myocardial ischaemia.
- High-sensitivity troponin assays and serial testing improve early diagnosis in suspected ACS.
- Do not delay reperfusion in obvious STEMI while waiting for troponin results.
- Many non-ACS conditions can elevate troponin, and these elevations are usually clinically meaningful rather than false positives.
- Troponin is most useful when interpreted together with symptoms, ECG findings, timing, and alternative diagnoses.
References
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction.
- Wu AHB, Christenson RH, Greene DN, et al. High-Sensitivity Cardiac Troponin and the 2021 AHA/ACC/ASE Chest Pain Guideline.
- MSD Manual Professional Edition. Overview of Acute Coronary Syndromes (ACS).
- American College of Cardiology. Causes of Non-ACS Related Troponin Elevations.
- ACC Accreditation Services. Guidelines for Troponin Testing.
Included image files
- Featured thumbnail hero image
- Troponin kinetics illustration
- Troponin interpretation flowchart
- STEMI ECG image
- NSTEMI ECG image