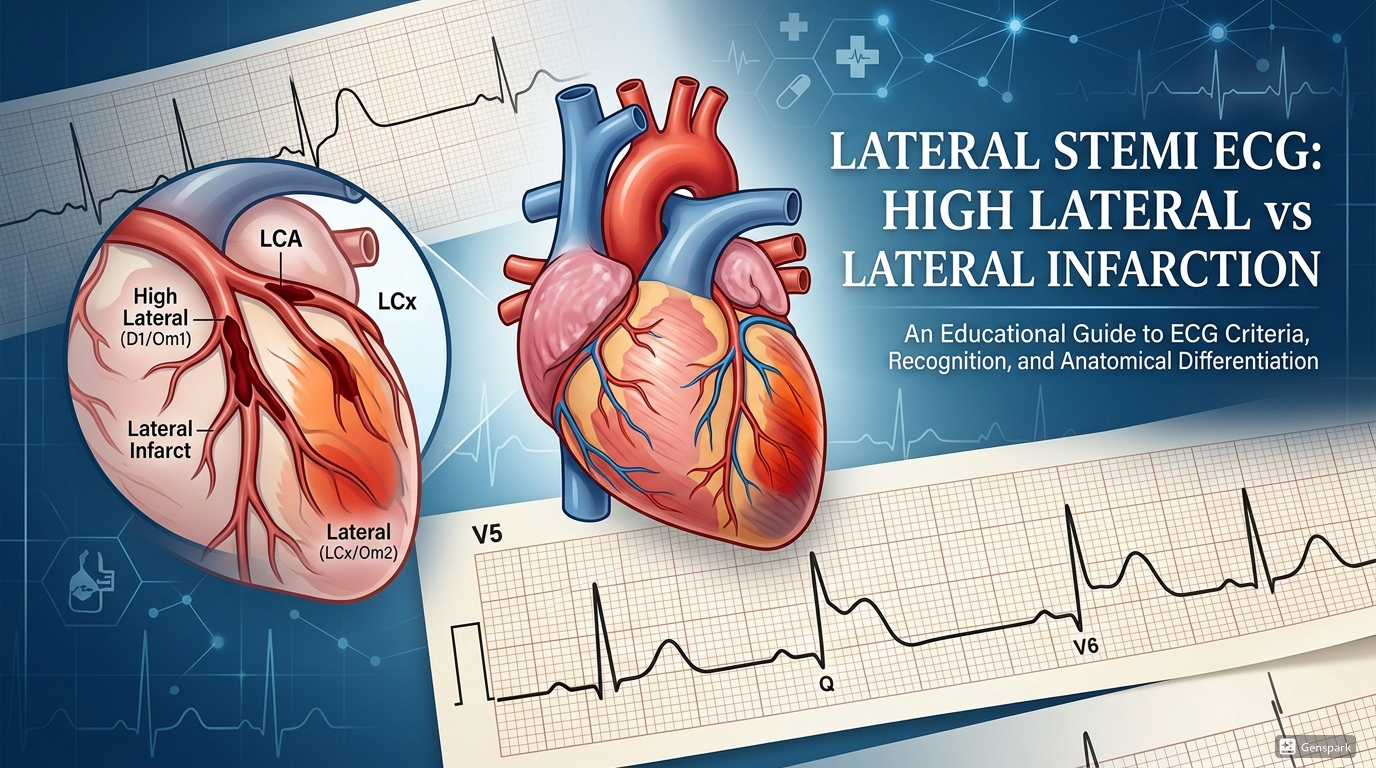
Lateral STEMI ECG: High Lateral vs Lateral Infarction
Description: Learn how to recognize high lateral and lateral STEMI on ECG, understand lead patterns in I, aVL, V5, and V6, identify reciprocal inferior changes, and think through likely culprit vessels.

|
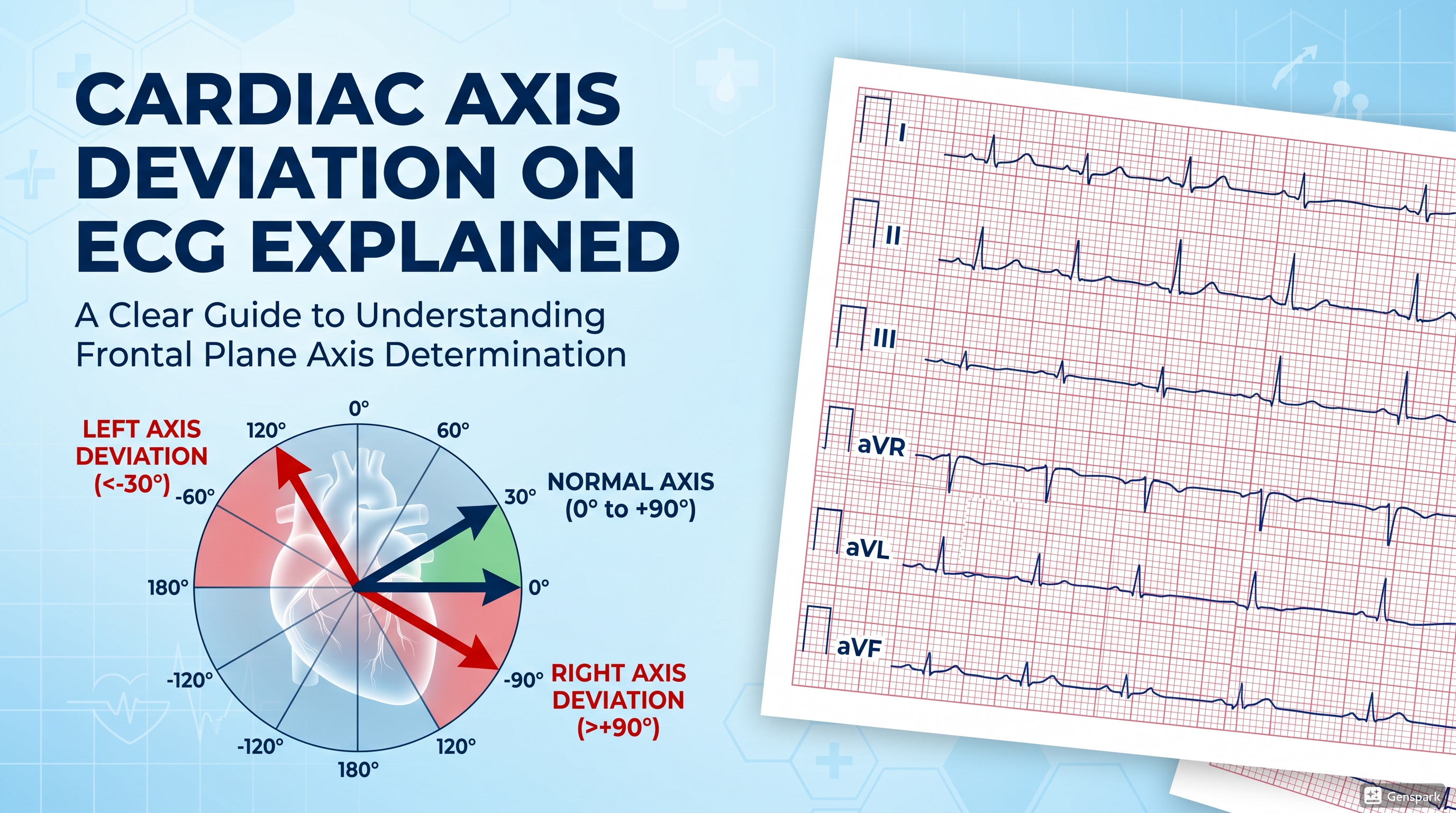
Quick answer: Lateral STEMI is recognized by ST-segment elevation in the lateral leads, classically I, aVL, V5, and V6, often with reciprocal ST depression in inferior leads III and aVF. High lateral STEMI is a more focused pattern in which ST elevation is mainly localized to leads I and aVL, sometimes with V2, and may suggest first diagonal branch occlusion. Broader lateral involvement including V5 and V6 suggests more extensive lateral wall infarction, often involving circumflex or obtuse marginal branches. |
Lateral STEMI is an ECG pattern that medical students and junior doctors often find harder to recognize than inferior or anterior infarction. The reason is simple: the involved leads are fewer, the ST elevation may be more subtle, and the territory can overlap with high lateral, anterolateral, or inferolateral patterns. Despite that, recognizing lateral infarction matters because it may represent occlusion of an important branch vessel, may occur with additional infarct territories, and can be easy to overlook if the clinician is focused only on the more familiar inferior or anterior leads.
A useful way to approach this topic is to separate high lateral STEMI from broader lateral STEMI. High lateral infarction is usually concentrated in leads I and aVL, sometimes with V2, while broader lateral infarction extends into V5 and V6. Once you recognize that distinction, the ECG becomes easier to read and the likely culprit artery becomes easier to think through.
Which leads look at the lateral wall?
The lateral wall is viewed by leads I, aVL, V5, and V6. Among these, leads I and aVL are often described as the high lateral leads, while V5 and V6 reflect the more lateral left ventricular wall. That is why isolated ST elevation in I and aVL is generally called high lateral STEMI, whereas ST elevation involving I, aVL, V5, and V6 points toward a broader lateral infarction.
This lead grouping is clinically useful because it gives structure to what might otherwise feel like a vague pattern. If you see ST elevation in I and aVL, ask whether V5 and V6 are involved too. That simple step often helps separate high lateral from lateral infarction.
Core ECG features of lateral STEMI
The classic ECG features of lateral STEMI are ST elevation in the lateral leads and reciprocal ST depression in the inferior leads, especially III and aVF. Reciprocal changes are important because they often make the diagnosis more convincing, especially when the ST elevation in the lateral leads is modest. In practice, ST depression in the inferior leads may only be obvious when there is clear ST elevation in I and aVL.
The main high-yield bedside lesson is to look for a lateral-inferior mirror relationship. If I and aVL are elevated while III and aVF are depressed, the tracing should immediately raise concern for lateral infarction.

What is high lateral STEMI?
High lateral STEMI is a more localized pattern in which ST elevation is mainly confined to leads I and aVL, sometimes with subtle involvement of V2. Reciprocal ST depression and/or T-wave inversion usually appears in the inferior leads and is often most obvious in lead III. This pattern is important because it can be mistaken for a minor or nonspecific abnormality if the clinician does not actively inspect I and aVL.
High lateral STEMI is strongly associated with occlusion of the first diagonal branch of the LAD. Teaching sources also describe the “South Africa Flag sign,” in which the distribution of ST elevation in I, aVL, and V2 together with inferior depression resembles the shape of the South African flag on a 4-by-3 ECG display. You do not need to rely on the visual mnemonic, but it can help learners remember the pattern.

High lateral vs lateral STEMI: how to tell the difference
The easiest distinction is the involvement of V5 and V6. If the ST elevation is primarily in I and aVL, think high lateral STEMI. If V5 and V6 are also involved, think broader lateral STEMI. In broader lateral infarction, the likely culprits may include obtuse marginal branches, the circumflex artery, ramus intermedius, or a more extensive lesion pattern depending on the accompanying territories.
It also helps to think in syndromic patterns. Isolated high lateral infarction often reflects smaller branch artery occlusion such as D1. Broader lateral infarction may occur as part of anterolateral STEMI due to LAD occlusion or inferoposterolateral infarction due to circumflex involvement. In other words, lateral STEMI is often a clue to the wider infarct map rather than an isolated diagnosis in every case.

Culprit artery clues
High lateral STEMI most classically points toward first diagonal branch occlusion. When the circumflex artery is the culprit, ST elevation in I and aVL may be accompanied by involvement of V5 and V6, producing a broader lateral picture. LITFL also groups lateral infarction into three broad patterns: anterolateral STEMI due to LAD occlusion, inferoposterior-lateral STEMI due to circumflex occlusion, and isolated lateral infarction due to smaller branch occlusion such as D1, obtuse marginal, or ramus intermedius.
These clues do not replace angiography, but they are valuable for ECG reasoning. They help the clinician move from “there is ST elevation” to “what territory and what likely vessel are involved?”
Why reciprocal inferior changes matter
Reciprocal ST depression in III and aVF is one of the most helpful supporting signs in lateral STEMI. It often sharpens your confidence that subtle ST elevation in I and aVL is not a benign variant. However, teaching sources point out an important exception: if there is simultaneous inferior ST elevation, as in inferolateral STEMI, the reciprocal pattern may be obscured or lost. That means absence of inferior reciprocal depression does not automatically rule out lateral infarction when multiple territories are involved.
How lateral STEMI overlaps with other infarct patterns
Lateral STEMI rarely exists in isolation in a purely academic way. It may overlap with anterior STEMI in anterolateral patterns or with circumflex-related inferoposterolateral infarction. This is why a full 12-lead review matters. If lateral leads are involved, you should also inspect the precordial and inferior leads carefully rather than stopping at the first abnormality you see.
For example, ST elevation in lateral leads plus high lateral leads can suggest a proximal LAD lesion in an anterolateral pattern. Conversely, lateral involvement with inferior changes can suggest circumflex territory extension. Thinking in territories rather than isolated labels leads to better ECG interpretation.
Why timing and repeat ECGs still matter
In suspected ACS, the ECG should be obtained and interpreted within 10 minutes of presentation. This matters because subtle lateral or high lateral STEMI can be missed early, especially when symptoms are typical but the initial tracing is not dramatic. A nondiagnostic first ECG does not exclude ACS, and repeat ECGs should be obtained if symptoms continue, recur, or the patient’s condition changes.
This is particularly relevant for lateral patterns because they are easier to overlook than classic inferior or extensive anterior STEMI. A careful comparison with prior ECGs and repeat tracing strategy can prevent missed reperfusion opportunities.

A practical bedside checklist
When you suspect high lateral or lateral STEMI, go through these steps:
- Look at I and aVL first for ST elevation.
- Check whether V5 and V6 are also involved.
- Look for reciprocal ST depression in III and aVF.
- Decide whether the pattern is isolated high lateral or broader lateral infarction.
- Think about likely culprit vessels such as D1, obtuse marginal, circumflex, or a broader LAD-related pattern.
- Review the rest of the 12-lead ECG for anterior, inferior, or posterior extension.
- Escalate promptly because any STEMI pattern may require urgent reperfusion.
Common mistakes to avoid
- Ignoring leads I and aVL because the more dramatic STEMI patterns are expected elsewhere.
- Missing subtle high lateral ST elevation when reciprocal inferior changes are actually the easiest clue.
- Calling all lateral ST elevation isolated when the tracing actually shows anterolateral or inferolateral involvement.
- Forgetting that absence of obvious inferior reciprocal depression does not exclude lateral STEMI when multiple territories are involved.
- Failing to repeat the ECG when symptoms are convincing but the first tracing is nondiagnostic.
Frequently asked questions
Which leads define high lateral STEMI?
High lateral STEMI is mainly defined by ST elevation in leads I and aVL, sometimes with V2 involvement.
Which leads define broader lateral STEMI?
Broader lateral STEMI involves the lateral leads I, aVL, V5, and V6.
What artery commonly causes high lateral STEMI?
A classic culprit is occlusion of the first diagonal branch of the LAD, although circumflex-related patterns can also involve I and aVL.
What reciprocal changes are most useful?
Reciprocal ST depression in leads III and aVF is the most useful supporting sign.
Why can lateral STEMI be missed?
Because the ST elevation may be subtle, localized to only a few leads, and overshadowed by attention to more familiar inferior or anterior STEMI patterns.
Key takeaways
- High lateral STEMI is mainly seen in leads I and aVL, sometimes with V2.
- Broader lateral STEMI involves I, aVL, V5, and V6.
- Reciprocal inferior ST depression in III and aVF is a key supporting clue.
- High lateral patterns often point toward first diagonal branch occlusion.
- Broader lateral involvement may suggest circumflex, obtuse marginal, ramus, or larger multiterritory infarct patterns.
- A nondiagnostic initial ECG does not exclude ACS, so repeat ECGs matter when suspicion remains high.
References
- High Lateral STEMI – ECG Library Diagnosis.
- Lateral STEMI – ECG Library Diagnosis.
- 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Diagnosis and Risk Classification of Acute Coronary Syndromes.
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction.